Low-Grade Serous Ovarian Cancer: Your Complete Guide to Diagnosis, Treatment & Hope
September 29, 2025

Low-grade serous ovarian cancer (LGSOC) is a rare subtype of ovarian cancer that often gets overshadowed by its more well-known counterpart, high-grade serous ovarian cancer. But just because it’s rare doesn’t mean it’s not important.
It’s time we put LGSOC in the spotlight and arm ourselves with the knowledge to fight back. When it comes to ovarian cancer, information isn’t just helpful; it’s essential, and we’re committed to sharing it.
Stay informed
Sign up to receive vital updates through email, and learn how you can get involved.
"*" indicates required fields
What Is Low-Grade Serous Ovarian Cancer (LGSOC)?
LGSOC (also known as low-grade serous carcinoma) is a type of epithelial ovarian cancer that accounts for less than 10% of all ovarian cancers. It’s a slow-growing cancer that doesn’t receive as much research attention as its more aggressive high-grade counterpart. The cells in LGSOC look more like normal tissue, which might sound reassuring. But this characteristic actually makes LGSOC harder to detect early on.
(Read more: LGSOC vs HGSOC: Understanding the Two Faces of Ovarian Serous Carcinoma)
Despite its slow growth, LGSOC can be just as invasive as high-grade cancer, silently spreading to nearby organs. It’s a formidable challenge that demands our attention and research efforts.
One thing to keep in mind is that LGSOC tends to affect younger women compared to high-grade serous ovarian cancer. According to ovarian cancer facts and research, the average age at diagnosis for LGSOC is around 45 years old, while for high-grade, it’s closer to 63. This means that LGSOC patients often face unique challenges, like balancing treatment with work, raising a family, managing fertility concerns, and dealing with early-onset menopause.
How Low-Grade Serous Ovarian Cancer Develops
Doctors, researchers, and scientists are still trying to piece together the puzzle of how LGSOC starts. It might come from the ovaries or the fallopian tubes. Some experts think it could develop step-by-step from borderline ovarian cancer or tumors (BOT), which are a type of ovarian tumor that’s not as invasive as traditional cancer.
What we do know is that certain gene changes, like KRAS and BRAF mutations, are often found in LGSOC cells. These changes are like a distinct molecular signature that sets LGSOC apart from other ovarian cancers.
But here’s the thing: not all LGSOC tumors have these mutations. Around 40% of LGSOC tumors don’t have identifiable mutations. This makes studying LGSOC even more challenging and critical. We must determine what makes these tumors tick to find better treatment methods.
Low-Grade Serous Ovarian Cancer Symptoms
LGSOC is notorious for flying under the radar. It’s often diagnosed at later stages when it has already spread beyond the ovaries.
The symptoms can be vague and mimic other common issues. Bloating, belly pain, feeling full quickly, and changes in peeing habits are all potential red flags. But here’s the thing: these symptoms can also show up in a myriad of other health conditions, from the most common gastrointestinal issues to other cancers. That’s why it’s so hard to detect LGSOC with symptoms alone. You really have to listen to your body and advocate for yourself if something doesn’t feel right.
Some women with LGSOC also report other symptoms, like fatigue, back pain, constipation, and pain during sex. These symptoms can be easy to brush off or attribute to other causes, but if they persist or get worse, it’s always best to get them checked out.
Diagnosing Low-Grade Serous Ovarian Cancer
Diagnosing LGSOC is like solving a complex mystery. An accurate LGSOC diagnosis takes a mix of different clues and tests. Imaging scans like ultrasounds, CT scans, and MRIs can give us a peek inside. The CA-125 blood test can also hint at ovarian cancer. This test measures the level of a protein called CA-125 (cancer antigen 125) in the blood. High levels can be a sign of ovarian cancer, but they can also be caused by other conditions, like endometriosis or fibroids.
Often, the definitive answer comes from a surgical biopsy, where doctors can examine the cells closely and determine whether it’s really LGSOC. During this procedure, the surgeon removes a small piece of tissue from the ovary or other suspicious areas. A pathologist then examines the cells under a microscope for the final diagnosis.
In some cases, doctors may also recommend somatic genetic testing to look for specific gene changes associated with LGSOC, like KRAS and BRAF mutations. This information can help guide ovarian cancer treatment decisions and give us a better understanding of the cancer’s behavior.
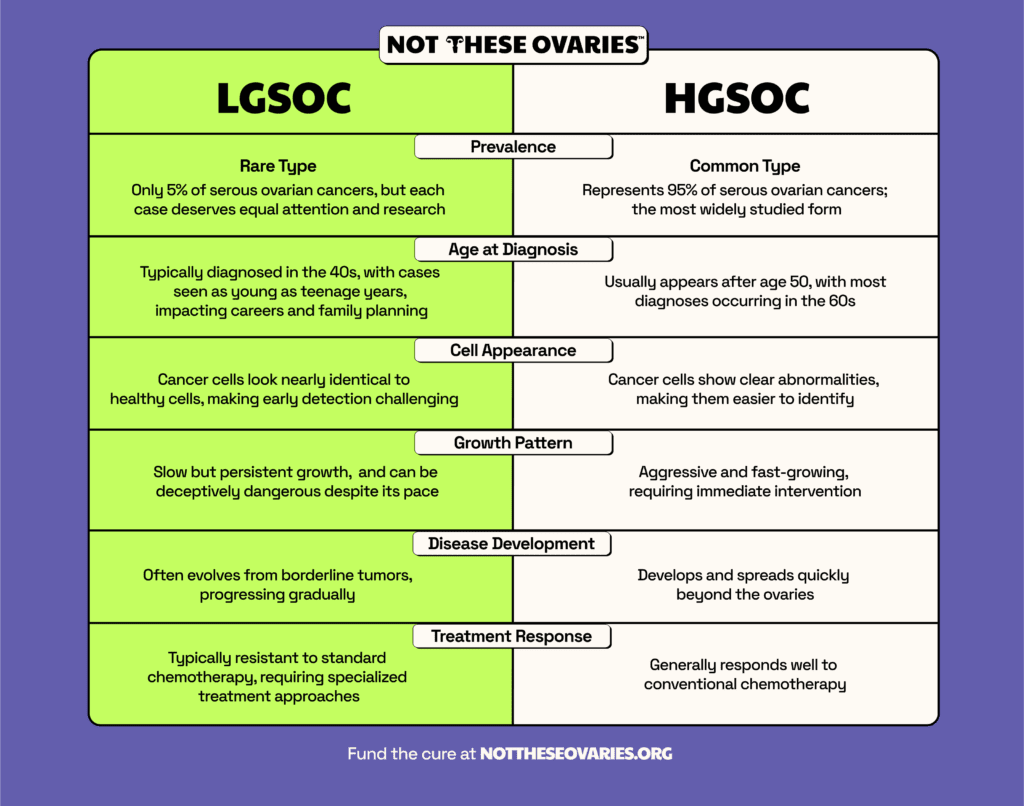
Differences Between Low-Grade and High-Grade Serous Ovarian Cancer

LGSOC and high-grade serous ovarian cancer (HGSOC) might sound similar, but their behaviors and appearances are very different.
Under the microscope, LGSOC cells show mild nuclear atypia, meaning they still somewhat resemble normal ovarian cells.
In contrast, HGSOC cells are almost unrecognizable from the ovarian cells from which they originated. These microscopic differences reflect their growth patterns, too: LGSOC cells are the slow-growing type, taking their time to spread, while HGSOC cells are more aggressive, multiplying and invading quickly.
While both types can share some genetic alterations, their mutation patterns tend to differ. LGSOC frequently has KRAS and BRAF mutations as key drivers. HGSOC is primarily characterized by BRCA and TP53 alterations, though it can also have KRAS mutations through the RAS pathway, albeit less commonly.
The most significant difference is how they respond to treatment. LGSOC tends to be far less sensitive to standard chemotherapy drugs compared to HGSOC. While chemotherapy might work well against HGSOC, it shows limited effectiveness in LGSOC patients.
In fact, chemotherapy for LGSOC is effective in fewer than 1 in 20 patients. Standard chemotherapy achieves tumor shrinkage in only 2 to 23% of LGSOC patients receiving neoadjuvant treatment, compared to 80 to 90% response rates for HGSOC. This stark difference underscores why we urgently need targeted, personalized treatments that work specifically for LGSOC.
Another key difference is survival rates. While HGSOC tends to grow and spread quickly, leading to poorer outcomes, LGSOC generally has a better prognosis. In one study, the median overall survival for advanced-stage LGSOC was 82 months, compared to 58 months for HGSOC. But it’s important to remember that every cancer is unique, and individual factors like age, overall health, and response to treatment can all impact survival.
(Learn more about LGSOC vs. HGSOC.)
Stages and Prognosis of Low-Grade Serous Ovarian Cancer
Like other ovarian cancers, LGSOC is staged from I to IV. Higher stages mean the cancer has spread further. The earlier LGSOC is caught, the better the chances of survival.
One study found that patients with stage II-IV LGSOC had a median overall survival of 82 months. That means half of the patients lived longer than 82 months. In contrast, patients with HGSOC had a median overall survival of 58 months. So, while LGSOC is no walk in the park, it generally has a better prognosis than its high-grade cousin. (This could also be due to age at diagnosis, with more cases of LGSOC in young women.)
But prognosis isn’t just about the numbers. Age, how much cancer is left after surgery, and the presence of certain gene changes can all impact survival. For example, being diagnosed at a younger age (35 or under) has been linked to worse outcomes in LGSOC. Conversely, having MAPK gene changes has been tied to better overall survival in some studies.
It’s also worth noting that LGSOC tends to have a higher recurrence rate than HGSOC. In one study, over 80% of patients with advanced LGSOC experienced a recurrence at some point.
But here’s what’s different about LGSOC recurrences: they typically grow more slowly than HGSOC recurrences, which can provide more time to plan treatment approaches. In some cases, surgical intervention alone may be effective in managing recurrence, though treatment options will depend on factors like where the cancer has returned and what therapies were used initially.
Low-Grade Ovarian Cancer Treatment Options
Surgery is the cornerstone when it comes to treating LGSOC. It is not optional, but rather a critical first step. The goal is to remove as much of the visible tumor as possible, as other treatments won’t work as effectively without tumor removal. This could mean a major surgery to debulk the cancer, a fertility-saving surgery for younger patients, or a second surgery if the cancer comes back.
Additional treatments are used alongside surgery, though their effectiveness varies. Chemotherapy, particularly carboplatin and paclitaxel, has shown limited success in LGSOC compared to HGSOC. Doctors must often follow this standard of care, especially in the United States, where insurance requirements can dictate treatment protocols.
The poor response rate to chemotherapy underscores why ovarian cancer clinical trials and research funding are crucial: we desperately need better options for LGSOC patients beyond traditional chemotherapy.
Hormone therapy, especially with drugs called aromatase inhibitors, has shown some promise in LGSOC. These meds work by blocking estrogen, which can fuel the growth of LGSOC cells. In one study, the response rate to hormone therapy in recurrent LGSOC was around 9%, with 61% of patients achieving stable disease. Research also showed that giving hormone therapy as maintenance after chemotherapy led to almost 40 months of progression-free survival.
Targeted therapies, like MEK inhibitors and BRAF inhibitors, are emerging treatment options. They zero in on specific gene changes often found in LGSOC, like KRAS and BRAF. In a phase II study of the MEK inhibitor selumetinib, 15% of patients with recurrent LGSOC had an objective response, and 65% achieved stable disease.
Let’s not forget the importance of LGSOC clinical trials. These are research studies testing new treatments and combinations to help improve outcomes and quality of life for LGSOC patients. Participating in a clinical trial gives you access to cutting-edge treatments and helps advance our understanding of LGSOC and how to treat it best.
Breakthrough Treatment: FDA-Approved Avutometinib and Defactinib
In a landmark development for LGSOC patients, the FDA granted accelerated approval in 2025 to AVMAPKI FAKZYNJA CO-PACK (avutometinib and defactinib) as the first-ever treatment specifically designed for adult patients with KRAS-mutated recurrent low-grade serous ovarian cancer who have received prior systemic therapy.
This groundbreaking oral combination therapy targets the specific genetic mutations that drive cancer growth in approximately 30% of LGSOC cases. The treatment works through a powerful dual mechanism: avutometinib blocks both the MEK and RAF signaling pathways that cancer cells use to grow, while defactinib (a FAK inhibitor) prevents cancer cells from developing resistance to the treatment.
What makes this approval truly exciting: In the Phase 2 RAMP 201 clinical trial with 57 adult patients, 44% of those with KRAS-mutated recurrent LGSOC experienced significant tumor shrinkage, as assessed by an independent review committee. This represents a dramatic improvement over standard chemotherapy response rates. Some patients saw their tumors shrink by 70% within just four months of starting treatment. Even more encouragingly, some patients continued to benefit from the treatment for over two years.
How the treatment works: Patients take avutometinib twice weekly and defactinib twice daily for three weeks, followed by a one-week break before resuming the cycle. While some patients experience side effects, the treatment has become the new standard of care for LGSOC patients with KRAS mutations.
This breakthrough didn’t happen overnight. The research behind this treatment began over a decade ago at Memorial Sloan Kettering Cancer Center, where scientists studying “exceptional responders” — rare patients who responded remarkably well to treatments — discovered how MEK1 protein defects drive LGSOC growth. Other research teams built on this discovery, finding that targeting FAK alongside MEK created a more effective, longer-lasting approach.
What this means for patients: If you have LGSOC, talk to your doctor about genetic testing for KRAS mutations to determine if this treatment might be appropriate for your situation. For women facing this rare cancer, having a treatment specifically designed for their exact type of LGSOC offers real hope where options were previously extremely limited.
(Learn more about avutometinib and defactinib.)
Managing Recurrent Low-Grade Serous Ovarian Cancer
 Recurrence is a common and frustrating part of the LGSOC journey. Unlike HGSOC, which often comes back within a couple of years, LGSOC can reappear many years after the first treatment. Studies show that over 80% of patients with advanced LGSOC will face a recurrence at some point.
Recurrence is a common and frustrating part of the LGSOC journey. Unlike HGSOC, which often comes back within a couple of years, LGSOC can reappear many years after the first treatment. Studies show that over 80% of patients with advanced LGSOC will face a recurrence at some point.
But LGSOC recurrence doesn’t mean game over. There are lots of ways to manage LGSOC when it rears its ugly head again. A combination of systemic treatments prescribed by your doctor like chemo, hormone therapy, and targeted drugs can all be used. In some cases, a second surgery to remove the cancer might be an option.
Focusing on quality of life is just as important as fighting cancer. Palliative care is all about easing symptoms and improving overall well-being. It’s not just about living longer but living better. This can include things like pain management, counseling, and spiritual support.
It’s also important to have open and honest conversations with your ovarian cancer doctor and medical team about your goals and priorities. Some people may choose to focus on aggressive treatment, while others may prioritize quality of life over quantity. There’s no right or wrong answer; it’s all about what matters most to you.
Coping with a Low-Grade Serous Ovarian Cancer Diagnosis
Getting diagnosed with LGSOC can be a total gut punch. Fear, anger, sadness, uncertainty: it’s a whole mess of emotions. But you don’t have to deal with it alone. There are lots of support resources out there, like counseling, support groups, and online communities. Lean on them when you need to.
Talking openly with your medical team is also key. Don’t be afraid to ask questions, speak up about your worries, and fight for what you need. Your doctors and nurses are there to guide you, but you’re the boss of your own body.
For younger patients, fertility might be a big concern. Talking with your care team about options like fertility-saving surgery or freezing your eggs can help you make decisions about your future family plans. Some women may also choose to explore alternative paths to parenthood, like adoption or surrogacy.
Remember, you’re not alone in this. Connecting with other LGSOC patients and survivors can give you a sense of community and hope. Their stories can be a shining light on the darkest days. And if you’re feeling up to it, consider sharing your story. You never know who you might inspire or help along the way.
The Future of Low-Grade Serous Ovarian Cancer Research
The future of LGSOC research holds genuine promise. One of the benefits of ovarian cancer clinical trials is that they are the driving force behind finding new treatments and improving outcomes. When patients participate in these trials, they help researchers unlock the mysteries of LGSOC and find better ways to beat it.
Some exciting areas of study include finding new ovarian cancer biomarkers to help guide treatment decisions, developing new imaging techniques for earlier detection, and exploring combination therapies to boost treatment effectiveness.
But the most important part of LGSOC research is the shared goal of improving the lives of people affected by this disease. Every study, trial, and breakthrough is a step towards better outcomes, better quality of life, and, one day, a cure.
Of course, research requires funding. That’s where organizations like Not These Ovaries come in. By donating to LGSOC research through our ovarian cancer research fund, you’re not just supporting scientific progress; you’re giving hope to the thousands of women and families affected by this disease. 100% of your donation goes directly to research. Not administrative costs, not marketing, but actual scientific investigation that can save lives. Every dollar counts, and together, we can make a real difference.
LGSOC may be a rare and challenging type of ovarian cancer, but it’s not insurmountable. With advances in research, FDA-approved targeted treatments, and a growing understanding of this complex disease, we’re making measurable progress in the fight against LGSOC.


