LGSOC vs HGSOC: Understanding the Two Faces of Ovarian Serous Carcinoma
December 6, 2024

In the realm of women’s health, few topics carry as much weight as ovarian cancer. This complex disease, often called the “silent killer,” affects thousands of women worldwide each year, making it a critical area of focus in gynecologic oncology. Understanding its nuances, particularly the crucial distinction between LGSOC vs. HGSOC, is not just a matter of medical interest — it’s a vital step towards more effective diagnosis and treatment strategies that can save lives and improve the quality of life for countless women.
Ovarian cancer is not a single disease but rather a group of distinct malignancies. The differences between LGSOC and HGSOC (low-grade serous ovarian carcinoma versus high-grade serous ovarian carcinoma) represent a crucial distinction in gynecologic oncology.
Though they affect the same organ, these two types of ovarian cancer are markedly different in their behavior, treatment response, and impact on patients’ lives. By delving into these differences, we gain invaluable insights that can shape the future of women’s healthcare and cancer treatment.
LGSOC vs HGSOC: The Fundamental Differences
Let’s unpack the complexities of LGSOC vs. HGSOC to better understand these two formidable opponents in the fight against ovarian cancer.
Stay informed
Sign up to receive vital updates through email, and learn how you can get involved.
"*" indicates required fields
Prevalence: Rarity vs. Commonality
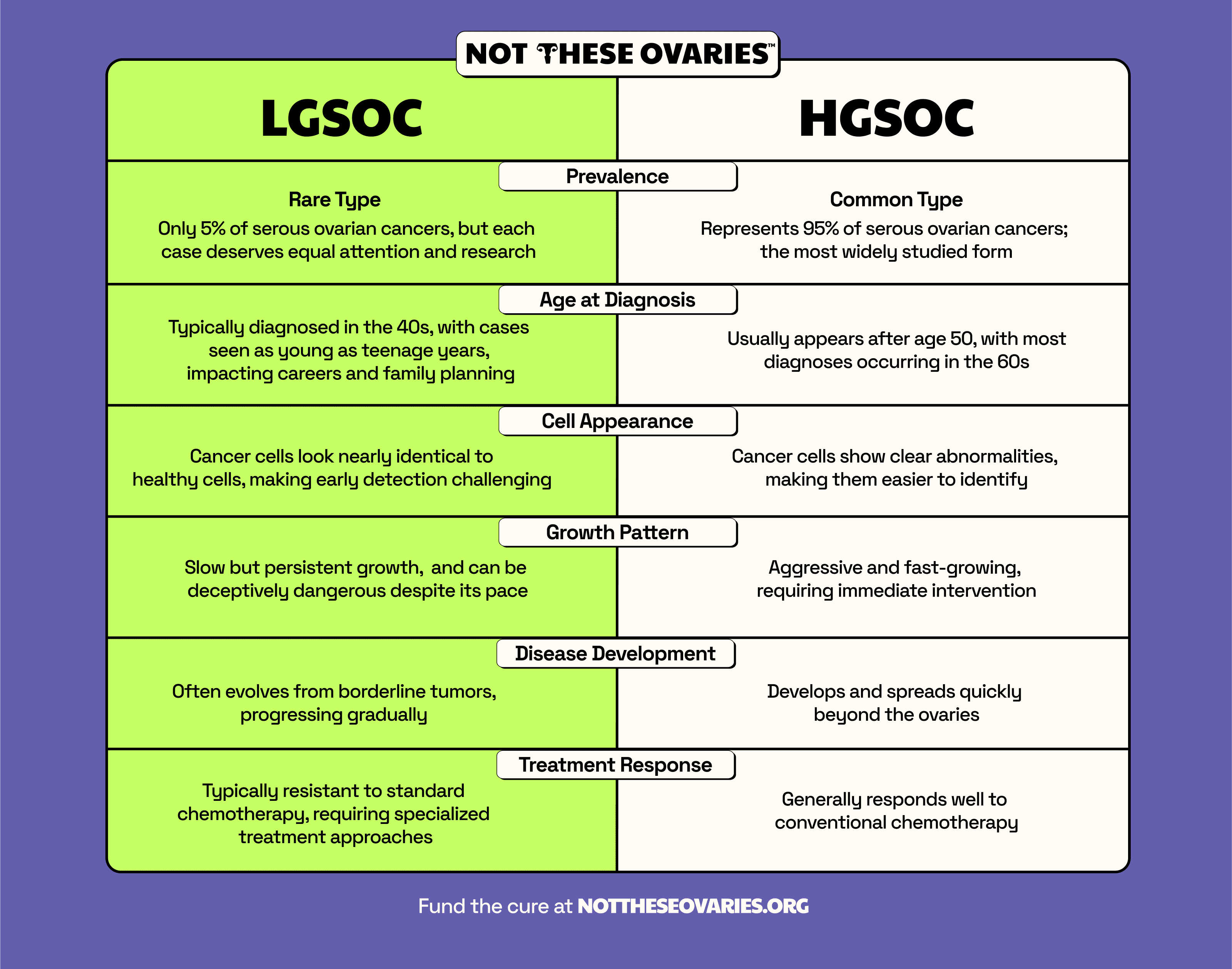
LGSOC is rare, making up only 5-10% of serous ovarian cancers. Its scarcity often challenges both patients and doctors. HGSOC, on the other hand, is much more common, accounting for 70-80% of all ovarian cancers. This significant difference in prevalence impacts research funding, treatment development, and clinical expertise.
Age at Diagnosis

LGSOC doesn’t discriminate by age. It often strikes women in their 40s and 50s (with the median age around 45 years old), but cases have been reported in patients as young as 14. Some women have even faced this LGSOC diagnosis in their teens, turning what should be carefree years into a battle for survival.
HGSOC typically appears later in life, with most diagnoses occurring in women between 55 and 65 years old. This age difference can profoundly impact ovarian cancer treatment decisions, fertility considerations, and overall life planning for patients.
Growth Patterns
LGSOC is a slow adversary. It often begins as a benign tumor, taking years to develop into a malignancy. This gradual progression offers a potential window for early detection and intervention, but it also means that patients may live with the disease for extended periods.
Conversely, HGSOC is aggressive and fast-moving. It can progress rapidly from early to advanced stages, often before symptoms become apparent. This swift progression makes early detection challenging and underscores the urgent need for improved screening methods.
Origin and Development
LGSOC often follows a stepwise progression from benign tumors to low-grade malignancy. This gradual evolution, known as the “Type I” pathway, can take years or even decades.
HGSOC typically develops rapidly, often appearing to arise de novo (arise suddenly from the beginning). Recent research suggests that many HGSOC cases may originate in the fallopian tubes rather than the ovaries.
In some studies, up to 48% of tumors initially interpreted as ovarian in origin contained a TIC (tubal intraepithelial carcinoma: lesions that are almost always detected in the fimbriated end of the fallopian tube) when all fallopian tube tissue was examined.
Genetic Profiles
LGSOC frequently harbors mutations in the KRAS and BRAF genes. These genes are like cellular on/off switches that control cell growth and division. When mutated, they get stuck in the “on” position, leading to uncontrolled cell growth. About two-thirds of LGSOC tumors carry one of these mutations.
HGSOC is predominantly characterized by mutations in the TP53 gene. TP53 is often called the “guardian of the genome” because it usually acts as a brake on cell division when DNA damage is detected. When TP53 is mutated, it can’t perform this protective function, allowing damaged cells to multiply unchecked. While most HGSOC cases show TP53 mutations, some rare cases may be TP53-negative while still showing abnormal p53 immunohistochemistry. This disruption of p53 function, whether through direct TP53 mutation or other mechanisms, contributes to the aggressive growth typical of HGSOC.
Understanding these genetic differences is crucial, as they influence how each type of cancer behaves and responds to treatment. They also provide targets for developing new, more precise therapies.
LGSOC vs HGSOC: Symptoms and Diagnosis
Despite their differences, LGSOC and HGSOC share many symptoms, making early diagnosis challenging. Common signs include:
- Abdominal bloating or swelling
- Feeling full quickly when eating (early satiety)
- Changes in bowel habits
- Intense back and pelvic pain
- Urgent need to urinate or increased frequency
- Abdominal or stomach pain
- Unexplained fatigue
- Symptoms that are ongoing for up to 2 weeks or more
The similarity of these symptoms to those of other conditions like irritable bowel syndrome or menstrual discomfort can lead to delayed diagnosis. This delay often results in both types of cancer being discovered at advanced stages.
The Diagnosis Challenge
Accurately diagnosing and differentiating between LGSOC and HGSOC typically involves a multi-step process:
- Pelvic exam
- Transvaginal ultrasound
- Blood tests (including CA-125 levels)
- Surgical intervention and biopsy
Surgery often becomes necessary not just for treatment but for definitive diagnosis. During the procedure, doctors aim to remove as much of the tumor as possible (debulking) and obtain samples for pathological examination.
The pathologist’s role is crucial in distinguishing between LGSOC and HGSOC through microscopic examination. LGSOC is characterized by mild to moderate nuclear atypia (cellular abnormalities) and a low rate of cell proliferation, while HGSOC shows marked nuclear atypia and high cell proliferation rates.
However, the subtle nature of LGSOC’s cellular changes can present a significant diagnostic challenge. These cells can be complex to identify precisely because they closely resemble normal cells and borderline ovarian tumors (BOTs). In contrast, HGSOC’s more pronounced cellular abnormalities make its detection more straightforward. This difference in detectability highlights why expert pathological examination is particularly crucial for LGSOC cases.
LGSOC vs. HGSOC: Treatment Response and Prognosis
 Regarding treatment and long-term outlook, LGSOC and HGSOC present different challenges and outcomes.
Regarding treatment and long-term outlook, LGSOC and HGSOC present different challenges and outcomes.
LGSOC tends to be stubborn, often resisting standard chemotherapy treatments. This resistance is a significant hurdle for doctors and patients, pushing researchers to explore alternative therapies.
Despite this challenge, LGSOC’s slower growth rate often translates to longer survival times. Many patients live with the disease for years, though they face the ongoing task of managing symptoms and maintaining their quality of life.
HGSOC, on the other hand, initially responds well to chemotherapy, particularly platinum-based regimens often combined with taxanes, offering a glimmer of hope at the start of treatment.
However, the long-term outlook remains challenging for two key reasons. First, chemotherapy resistance often develops over time in HGSOC cases. Second, early diagnosis or early detection of ovarian cancer is unfortunately rare, with many cases discovered at later stages, significantly impacting survival rates despite the initial good response to treatment.
In both cases, the journey is far from easy. While LGSOC patients might have more time, they face a marathon of symptom management. HGSOC patients, in contrast, often face a more intense, sprint-like treatment experience. Regardless of the type, these cancers underscore the critical need for early detection and innovative treatments to improve outcomes for all ovarian cancer patients.
This is why Not These Ovaries (NTO) supports LGSOC research. Recognizing the unique challenges posed by this form of ovarian cancer, NTO is committed to funding cutting-edge studies and clinical trials specifically targeting LGSOC.
By concentrating efforts on this underserved area, NTO aims to accelerate the development of more effective treatments, improve early detection methods, and ultimately enhance the quality of life for LGSOC patients. Through this dedicated approach, NTO is not just offering hope; it’s actively working to change the landscape of LGSOC treatment and care.
Treatment Strategies: LGSOC vs. HGSOC
The distinct characteristics of LGSOC and HGSOC necessitate different treatment approaches. Understanding these differences is crucial for both patients and healthcare providers.
LGSOC Treatment
LGSOC treatment involves several strategies tailored to each patient’s unique situation.
- Surgery is often the first step, aiming to remove as much of the tumor as possible. For younger patients, fertility-sparing surgery options may be available.
- Following surgery, adjuvant chemotherapy with carboplatin and paclitaxel is the standard of care for LGSOC patients, even when the disease is limited to the ovary. While LGSOC is relatively chemoresistant compared to HGSOC, this combination remains the established first-line treatment approach.
- Many LGSOC tumors are hormone-sensitive. Doctors use hormonal therapies, like aromatase inhibitors, to block estrogen’s effects on cancer cells. These are particularly useful for managing recurrent disease.
- As we learn more about LGSOC’s genetic profile, targeted therapies show promise. MEK inhibitors, which target a specific pathway often dysregulated in LGSOC, have shown encouraging results in clinical trials.
- Unlike HGSOC, LGSOC tends to be less responsive to traditional ovarian cancer chemotherapy. However, it’s still used in advanced cases or when other options have been exhausted.
This multi-pronged approach allows medical teams to adapt their strategies as needed. While challenges remain, ongoing research aims to improve treatments and outcomes for LGSOC patients.
Genetic testing has become a crucial tool in the fight against both LGSOC and HGSOC. It helps identify targetable mutations, guiding treatment decisions such as using PARP inhibitors. Moreover, it can reveal hereditary cancer syndromes, providing valuable information not just for patients but also for their family members who may be at increased risk.
 Despite advances in treatment, both LGSOC and HGSOC present significant challenges. Chemoresistance remains a significant consideration, with LGSOC showing relative resistance compared to HGSOC, though standard chemotherapy is still a necessary part of treatment. High recurrence rates necessitate ongoing monitoring and multiple treatment lines, while side effects can significantly impact quality of life. LGSOC’s rarity also means fewer established treatment options compared to HGSOC.
Despite advances in treatment, both LGSOC and HGSOC present significant challenges. Chemoresistance remains a significant consideration, with LGSOC showing relative resistance compared to HGSOC, though standard chemotherapy is still a necessary part of treatment. High recurrence rates necessitate ongoing monitoring and multiple treatment lines, while side effects can significantly impact quality of life. LGSOC’s rarity also means fewer established treatment options compared to HGSOC.
These challenges underscore the importance of personalized medicine in ovarian cancer care. By tailoring strategies to each cancer type and individual patient needs, doctors can provide more effective treatment. Ongoing research, particularly in immunotherapy and targeted treatments, offers hope for improved outcomes in the future.
Living with LGSOC and HGSOC: Quality of Life Considerations
Living with LGSOC or HGSOC presents unique challenges that extend beyond medical treatment.
LGSOC patients often face a longer journey, managing the disease for many years. This can lead to chronic stress and anxiety about recurrence, as well as significant impacts on fertility planning and career trajectories.
HGSOC patients, on the other hand, often experience more intense treatment periods and rapid life changes due to the aggressive nature of the disease. They may also need to confront end-of-life planning earlier in their journey.
One of the benefits of ovarian cancer clinical trials is the role they play in advancing treatment for both types of cancer. They offer patients access to cutting-edge treatments and contribute valuable knowledge to the field. For LGSOC, in particular, clinical trials are essential for developing new treatments due to their rarity. Many current trials explore novel combination therapies, which may prove more effective than single-agent treatments.
LGSOC and HGSOC: The Importance of Distinction
Understanding the differences between LGSOC and HGSOC is more than an academic exercise. It has real-world implications for diagnosis, treatment, and patient outcomes. By recognizing these two distinct entities, we can:
- Develop more targeted therapies
- Design clinical trials that address the unique challenges of each subtype
- Provide patients with more accurate prognoses and treatment expectations
- Allocate research resources more effectively
Knowledge is power in the fight against ovarian cancer, and understanding the distinctions between LGSOC and HGSOC empowers patients to participate actively in their care. Organizations like Not These Ovaries are leading the charge toward personalized care and improved outcomes, with a particular focus on advancing LGSOC research. By supporting NTO’s ovarian cancer research fund, you’re not just helping individual patients—you’re contributing to a broader mission that impacts families, communities, and the future of women’s health worldwide.



