LGSOC vs BOT: Understanding Two Distinct Ovarian Tumors
October 11, 2025

When you hear “borderline,” you might think “not serious.” When it comes to ovarian tumors, nothing could be further from the truth. Borderline ovarian tumors and low-grade serous ovarian cancer occupy a confusing middle ground that affects thousands of young women worldwide, and understanding the differences could literally save lives.
Understanding the differences between these two types of ovarian growths is crucial for proper diagnosis, treatment, and long-term health outcomes. Let’s dive deep into the world of low-grade serous ovarian cancer (LGSOC) and borderline ovarian tumors (BOT, or borderline ovarian cancer) to shed light on these complex conditions.
Stay informed
Sign up to receive vital updates through email, and learn how you can get involved.
"*" indicates required fields
What are LGSOC and BOT?
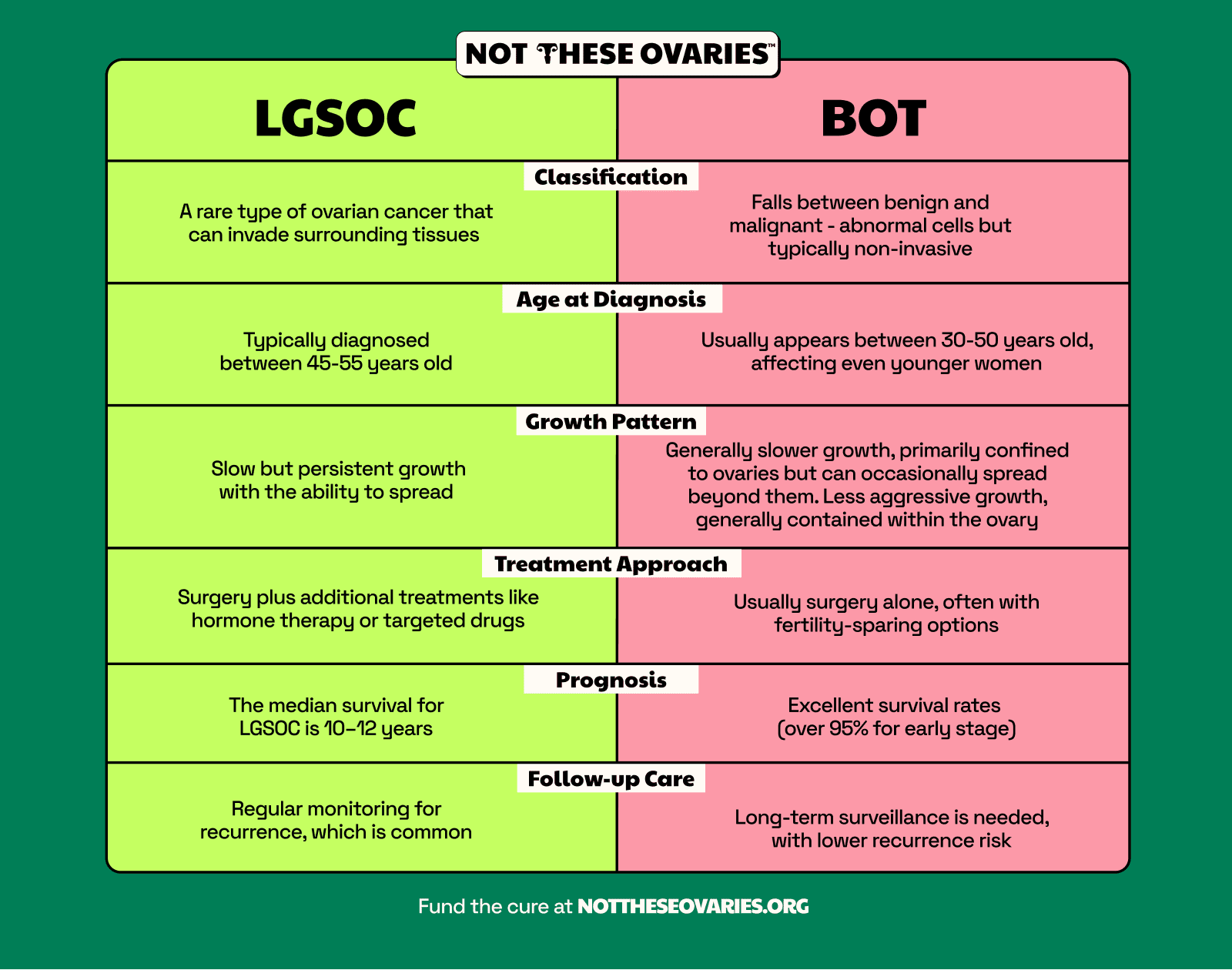
Low-grade serous ovarian cancer (LGSOC) is a rare subtype of ovarian cancer, representing approximately 2% of all epithelial ovarian cancers and accounting for about 4.7% to 10% of serous ovarian cancer cases. It’s characterized by slow growth and a distinct molecular profile that sets it apart from its more aggressive counterpart, high-grade serous ovarian cancer. LGSOC typically affects younger women and presents unique challenges in terms of treatment and management. (Read more about LGSOC vs. HGSOC.)
Borderline ovarian tumors (BOT), on the other hand, occupy a unique space in the spectrum of ovarian neoplasms. These tumors fall between benign and malignant classifications, exhibiting some characteristics of cancer cells but lacking the ability to invade surrounding tissues. It’s important to note that while they’re often referred to as “borderline,” these tumors can still pose significant health risks and require careful management.
The BOT-to-LGSOC Connection: What Research Shows
The relationship between LGSOC and BOT is an area of ongoing research and debate within the medical community.
Some experts believe that LGSOC could potentially develop from BOT, particularly in cases where BOT recurs. Research indicates that approximately 6.8% of borderline ovarian tumors recur as LGSOC. Studies also show that about 8.7% of LGSOC cases had transformed from serous borderline ovarian tumors. While the majority of BOT recurrences remain borderline — with recurrence rates of 5% to 25% depending on stage — the small percentage that progresses to LGSOC underscores the importance of long-term surveillance.
This connection doesn’t mean every BOT will progress to LGSOC, but it highlights the importance of careful monitoring and follow-up for patients diagnosed with BOT.
(Read more about the causes of low-grade serous ovarian cancer.)
The Age Factor: Who’s at Risk?
Age plays a significant role in the occurrence of both LGSOC and BOT, with these conditions typically affecting younger women compared to other types of ovarian cancer.
For borderline ovarian tumors, the highest prevalence occurs in women aged 40 to 49 years, with about one-third of patients diagnosed under age 40. LGSOC demonstrates a bimodal age distribution, with two distinct peaks of diagnosis occurring between ages 20 to 30 and again between 50 to 60. The average age at LGSOC diagnosis is 45 to 55.5 years, notably younger than the 62.6-year average for high-grade serous ovarian cancer.
This age difference is crucial because it impacts various aspects of patient care and quality of life. Younger women diagnosed with LGSOC or BOT often face unique challenges related to fertility preservation, treatment decisions, and long-term health planning. For many, the diagnosis comes at a time when they’re building careers, starting families, or planning for the future, adding an extra layer of complexity to their medical journey.
The younger age of onset also means that patients may be living with these conditions or their aftermath for many years, emphasizing the need for long-term care strategies and ongoing research into improving outcomes and quality of life for survivors.
Recognizing the Signs: Symptoms and Diagnosis
 One of the biggest challenges in identifying LGSOC and BOT early is that their symptoms can be vague and easily attributed to other, more common conditions.
One of the biggest challenges in identifying LGSOC and BOT early is that their symptoms can be vague and easily attributed to other, more common conditions.
Both LGSOC and BOT often present with symptoms such as abdominal bloating or swelling, pelvic pain, feeling full quickly when eating, and urinary symptoms like urgency or frequency. These nonspecific symptoms can often lead to delayed diagnosis, as they might be dismissed as menstrual issues, digestive problems, or simply signs of aging.
Here’s what’s alarming: research reveals that nearly all women with LGSOC — 99% — had never heard of the condition before diagnosis. Even more concerning, 65% believe they would have been diagnosed sooner if they had known more about it. The average time from symptom onset to diagnosis is nearly three years, with 68% of women reporting their symptoms were wrongly attributed to other conditions like irritable bowel syndrome or stress.
The diagnostic process for LGSOC and BOT typically involves a combination of methods. Initially, doctors may perform physical exams and order blood tests, including the CA-125 test, which can be elevated in ovarian cancers and some benign conditions. Imaging studies such as ultrasounds, CT scans, or MRIs are often used to visualize the ovaries and surrounding tissues.
However, the definitive diagnosis comes from a biopsy, where tissue samples are examined under a microscope. This is where the key differences between LGSOC and BOT become apparent. LGSOC cells show signs of invasion into surrounding tissues, while BOT cells look abnormal but haven’t invaded nearby structures.
Micropapillary Serous Borderline Ovarian Tumors: A Special Note
It’s worth noting that there’s a subtype of BOTs called micropapillary serous borderline ovarian tumors (MPSBOTs). These tumors occupy a gray area, showing more aggressive features than typical BOTs. MPSBOTs are associated with higher rates of bilateral ovarian involvement, recurrence, and invasive peritoneal implants. The 2014 WHO guidelines clarify that when these tumors show invasive implants that infiltrate underlying tissue, they should be classified as low-grade serous carcinoma rather than borderline tumors. (Read more: “Microinvasion in Borderline Ovarian Tumors: What You Need to Know“)
This distinction is crucial for determining the appropriate treatment approach and prognosis.
It’s worth noting that the diagnosis of BOT can sometimes be challenging, even for experienced pathologists. In some cases, what’s initially diagnosed as BOT may later be reclassified as LGSOC upon further examination or if the disease progresses. Conversely, there are instances where an initial LGSOC diagnosis might be reclassified as BOT after a more thorough review. This underscores the importance of having tissue samples reviewed by pathologists with expertise in gynecologic cancers.
Treatment Approaches: Tailoring Care to the Diagnosis
The treatment strategies for LGSOC and BOT differ significantly, reflecting the distinct nature of these two conditions.
LGSOC Treatment: A Multi-Faceted Approach
For LGSOC, surgery is typically the cornerstone of treatment. This often involves a comprehensive procedure to remove the ovaries, fallopian tubes, and uterus, along with any visible tumor deposits.
The goal is to achieve complete cytoreduction, meaning no visible disease is left behind after surgery. In some cases, especially for younger women who wish to preserve fertility, less extensive surgery might be considered if the disease is caught early.
Following surgery, many LGSOC patients receive chemotherapy. However, it’s important to note that LGSOC is notoriously resistant to traditional chemotherapy regimens. The response rates to chemotherapy for LGSOC are much lower than those seen in high-grade serous ovarian cancer, leading researchers to explore alternative treatment strategies.
One promising area of research in LGSOC treatment is hormonal therapy. Many LGSOCs are hormone-sensitive, and drugs that block estrogen or progesterone have shown some efficacy in controlling the disease. Recent studies have demonstrated that using hormone blockers after initial treatment can significantly delay recurrence in some patients.
Targeted therapies are another exciting frontier in LGSOC treatment. MEK inhibitors, which target specific mutations found in many LGSOC tumors, have shown promise in clinical trials. These drugs work by blocking signals that cancer cells use to grow and divide, potentially offering a more tailored approach to treatment.
Breakthrough LGSOC Treatment on the Horizon
There’s genuinely exciting news for LGSOC patients. A groundbreaking combination therapy of avutometinib and defactinib has shown remarkable results in clinical trials.
The FDA approved avutometinib and defactinib based on results from the Phase 2 RAMP 201 trial, which tested the combination in 57 adult patients with KRAS-mutated recurrent LGSOC. Here’s what the trial showed:
- Nearly half of the patients responded to treatment: 44% of patients saw their tumors shrink significantly
- Complete disappearance in some cases: 3.5% of patients had their tumors completely disappear
- Partial shrinkage in many: 4 out of 10 of patients had their tumors shrink by at least 30%
- Long-lasting benefits: Patients who responded maintained their benefits for anywhere from 3.3 months to over 2.5 years
In simpler terms, this drug combination works like a double barrier: one drug blocks the cancer’s main growth pathway, while the second drug prevents the cancer from finding a workaround, making it much harder for the cancer cells to survive and spread.
The treatment is specifically approved for and particularly effective in LGSOC patients with KRAS mutations, and whose cancer has returned, which accounts for approximately 30% of LGSOC cases. These mutations are common drivers of this cancer, making these patients ideal candidates for this targeted therapy approach.
BOT Treatment: Conservative When Possible
The treatment approach for BOT is generally less aggressive than that for LGSOC, reflecting its less invasive nature. Surgery is still the primary treatment, but it’s often less extensive than what’s required for LGSOC. Many women with BOT can have fertility-sparing surgery if desired, preserving the uterus and sometimes one ovary.
Chemotherapy is generally not recommended for BOT, as these tumors don’t respond well to traditional chemotherapy agents. Instead, the focus is on careful monitoring after surgery to detect any recurrence early. This typically involves regular follow-up visits, imaging studies, and blood tests to track CA-125 levels.
For both LGSOC and BOT, the importance of being treated at a center with expertise in gynecologic cancers cannot be overstated. The rarity of these conditions means that many general oncologists and OB-GYNs (obstetrician-gynecologists) may have limited experience in managing them, potentially impacting treatment decisions and outcomes. Consider consulting a gynecologic oncologist who specializes in these rare subtypes.
Prognosis and Survival: What to Expect
When it comes to prognosis and survival, LGSOC and BOT present different outlooks, reflecting their distinct biological behaviors.
LGSOC, while generally less aggressive than high-grade serous ovarian cancer, is still a serious malignancy. It’s characterized by slow but persistent growth, and patients often live with the disease for many years. The 5-year survival rate for LGSOC is better than that of high-grade serous ovarian cancer, but exact figures can vary depending on the stage at diagnosis and other factors.
One of the challenges with LGSOC is its tendency to recur, even years after initial treatment. Many patients find themselves dealing with multiple LGSOC recurrences over time, necessitating ongoing treatment and management. This long-term nature of the disease can have a significant impact on quality of life and requires a comprehensive approach to care that addresses both physical and emotional needs.
BOT, on the other hand, generally has a more favorable prognosis. The 5-year survival rate for early-stage BOT is over 95%, and even in cases where the disease has spread beyond the ovaries, the outlook remains generally good. However, it’s crucial to remember that BOT is not a benign condition and still requires careful management and follow-up.
One of the key concerns with BOT is the potential for recurrence and, in some cases, progression to LGSOC. While most BOT recurrences are still borderline, the possibility of malignant transformation underscores the need for long-term surveillance. Patients with BOT need to be vigilant about follow-up care and report any new symptoms promptly to their healthcare team.

Living with LGSOC or BOT: Beyond Medical Care
A diagnosis of LGSOC or BOT impacts far more than just a patient’s physical health. It can affect every aspect of life, from relationships and work to self-image and future plans. This is particularly true given that these conditions often affect younger women who may be in the midst of building careers, starting families, or planning for the future.
For many women diagnosed with LGSOC or BOT, fertility concerns are paramount. The potential need for extensive surgery, including removal of the ovaries and uterus, can have profound implications for family planning.
Some women may need to make quick decisions about egg freezing or other fertility preservation options before starting treatment. The possibility of treatment-induced early menopause is another significant concern that can affect long-term health and quality of life.
The emotional impact of an LGSOC or BOT diagnosis shouldn’t be underestimated. Patients often grapple with feelings of anxiety, depression, and uncertainty about the future. The chronic nature of LGSOC, with its potential for multiple recurrences, can be particularly challenging, as patients may feel like they’re living with a constant threat hanging over them.
Support systems play a crucial role in helping patients navigate these challenges. Support groups, whether in-person or online, can provide invaluable connections with others who understand the unique challenges of living with LGSOC or BOT. Mental health resources, including counseling and therapy, can help patients develop coping strategies and work through the emotional aspects of their diagnosis.
It’s also important for patients to maintain open communication with their healthcare team. This includes not just oncologists and surgeons, but also mental health professionals, fertility specialists, and other experts who can provide comprehensive care. Patients should feel empowered to ask questions, express concerns, and participate actively in decisions about their care.
Not These Ovaries: Championing LGSOC and BOT Research
At Not These Ovaries, we’re on a mission to drive forward LGSOC and BOT research. Our focus is clear: funding innovative studies and clinical trials, fostering collaboration among researchers worldwide, raising awareness about these rare conditions, and empowering patients with resources and support.
We believe that every patient deserves hope, no matter how rare their condition might be. Our goal is to improve treatments, enhance outcomes, and ultimately find a cure for LGSOC and BOT. By donating to our ovarian cancer research fund, you directly contribute to breakthrough studies and life-changing clinical trials.


